Note this case contains graphic images from surgery.
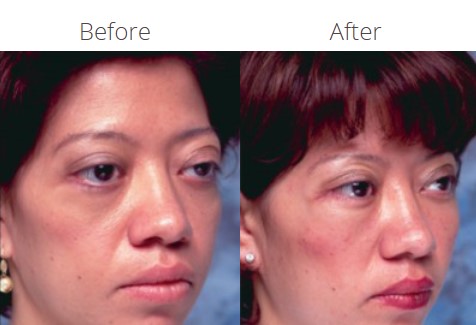
Chief Concern: This 28-year old has a history of childhood thyroid eye disease. She had orbital decompression at the Jules Stein Eye Institute as well as several other eyelid procedures. However, she has difficulty closing the eyelids.
Diagnosis: The patient had a profound benefit from her prior orbital surgery. However, she manifests poor projection of the inferior orbital rim. Consequently there is poor support for the lower eyelid and cheek. The lower eyelids hang below the curvature of the eyes. This prevents the eyelids from meeting upon lid closure.
Treatment:

The inferior orbital rim needs to be built up to support the cheek, which is vertically lifted onto the implant used along the orbital rim (Figure 2).
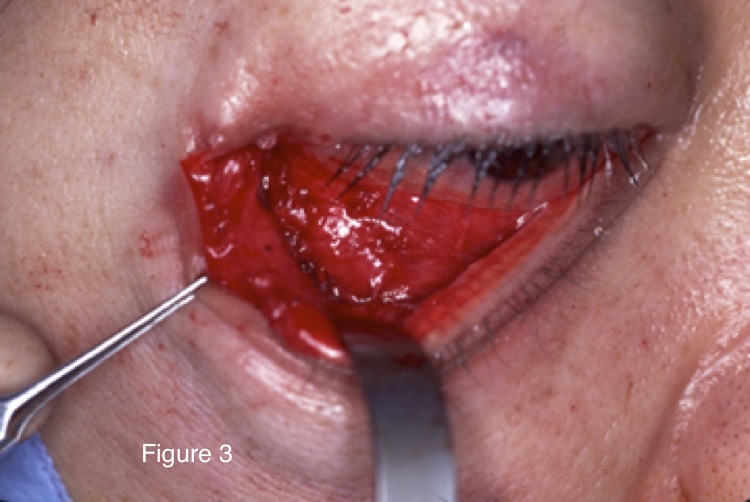
The midface is exposed through a swinging eyelid approach (Figure 3).
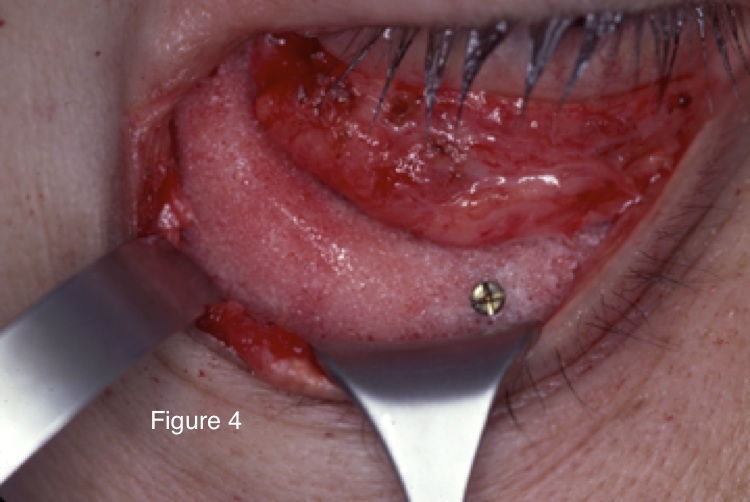
The implant is inserted and fixed to the orbital rim with microscrews (Figure 4).
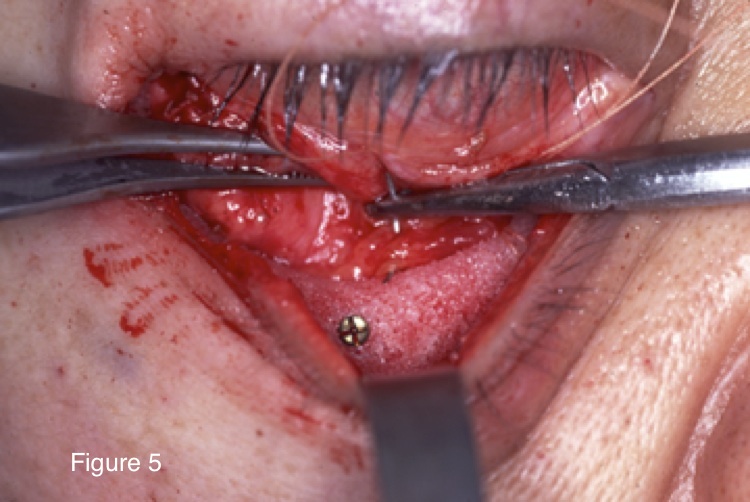
The cheek soft tissue is then vertically elevated to the top of the implant and fixed with stitches (Figure 5).

Hard palate graft is harvested from the roof of the mouth and used behind the lower eyelid to help lengthen it (Figure 6).

The lateral canthus is then resuspended and the skin is closed (Figure 7). Because the eyelids are immobilized and patched closed for a week to permit healing, only one side is done at a time. The other side was done 10 days later.
Before

After
